
FALCINE MENINGIOMA
FALX MENINGIOMA
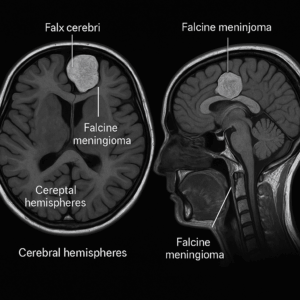
Falcine (Falx) Meningioma: Overview
Falcine meningiomas arise from the falx cerebri, the midline dural fold that separates the two cerebral hemispheres. As these deep, midline tumors enlarge, they press on the inner surfaces of the hemispheres and may trigger brain swelling (edema). Consequently, patients can develop neurologic symptoms and functional decline. These tumors most often occur along the falx in the frontal, parietal, or occipital regions.
Presentation
Symptoms depend on tumor location and growth.
-
Frontal falcine meningioma (mid-falx): Patients often experience focal motor or sensory seizures on the contralateral side. They may also develop progressive foot and leg weakness or sensory loss.
-
Occipital falcine meningioma (posterior falx): Patients may notice loss of peripheral vision on the side opposite the tumor.
Because the tumor sits at the midline, symptoms frequently affect both legs and may worsen as edema increases.
Management
Treatment is individualized and evidence-guided.
-
Surgery: Clinicians generally recommend microsurgical resection for symptomatic falx meningiomas to relieve pressure and control seizures.
-
Surveillance: Teams may observe small–medium, incidental tumors without edema, using scheduled MRI scans.
-
Radiation therapy: In older patients with small–medium tumors and mild symptoms without significant mass effect, physicians may offer CyberKnife® or proton-beam therapy.
Surgical Challenges
Surgeons plan carefully due to:
-
Exact localization requirements
-
Deep midline corridor
-
Edematous or tight brain
-
Tumor size/consistency
-
Nearby eloquent cortex (motor/sensory)
-
Proximity to feeding arteries and midline veins
Surgical Management at the Meningioma Center
At the Center for Meningioma Surgery, we tailor a small, midline craniotomy to tumor size and position. Using computer-assisted navigation (StealthStation™ or Brainlab), we pinpoint the lesion and minimize exposure. When edema is significant, we may choose a contralateral approach to avoid manipulating compromised brain. Under an operative microscope, we elevate the tumor along natural planes, debulk it with an ultrasonic aspirator, and then remove it piecemeal. We routinely coagulate/resect the falx dural origin and address any contralateral extension, which maximizes the chance of complete resection while protecting function.
Prognosis
With focused craniotomies and meticulous microsurgery, patients often achieve maximal tumor removal and preservation or recovery of motor function. Pre-operative seizures frequently come under control, sometimes with reduced medication. Moreover, smaller openings typically shorten operative time, reduce soft-tissue trauma and pain, and decrease hospital stay. Ultimately, comprehensive management supports a return to work and daily life. Maximizing resection—including the falx dural attachment—lowers recurrence risk and improves long-term tumor control.
Falcine (Falx) Meningioma Frequently Asked Questions:
Symptoms, Diagnosis & Imaging
What is a falcine (falx) meningioma?
A falcine meningioma arises from the falx cerebri, the membrane that separates the brain’s hemispheres. As it enlarges, it presses on nearby cortex and midline veins.
Which symptoms should I watch for?
Patients commonly notice headaches or seizures. In addition, the tumor may cause leg weakness, numbness, or changes in focus and personality—often affecting both legs because of the midline location.
How do doctors confirm the diagnosis?
Your team performs a neurologic exam and orders an MRI with contrast. Next, they may add CT to evaluate calcification and bone and to plan surgery.
Why does venous anatomy matter?
These tumors often abut the superior sagittal sinus. Therefore, surgeons map venous drainage on MRI/MRV to reduce the risk of postoperative swelling or venous injury.
Do all falx meningiomas need treatment right away?
Not necessarily. If the tumor is small and silent, clinicians may recommend active surveillance. However, growth, seizures, or progressive deficits usually prompt intervention.
Treatment, Recovery & Outcomes
What are my treatment options?
Your surgeon typically offers microsurgical resection. Alternatively, stereotactic radiosurgery treats small or residual tumors. When appropriate, careful surveillance monitors stable lesions.
How does surgery help?
Surgery decompresses the brain and removes tumor. When safe, the team also coagulates or resects the dural attachment on the falx to lower recurrence.
When is radiosurgery a good choice?
Radiosurgery works best for small, well-defined tumors that sit away from critical veins. Additionally, it controls residual or recurrent disease after surgery.
What results can I expect?
Many patients regain leg strength and reduce seizures. As a result, day-to-day function often improves, especially with early treatment.
What does recovery involve?
Most patients stay 1–3 days in the hospital and resume light activity in 2–4 weeks. Finally, scheduled MRIs and clinic visits track healing and detect recurrence early.